
PAD Trial Results Make the Case for Training Volunteers to Use AEDs
Police Expand Defibrillator Program to Each Precinct
September 16, 2003SAVING LIVES
December 3, 2003November 17, 2003 — Results of the Public Access Defibrillation (PAD) trial suggest that the number of survivors of out-of-hospital cardiac arrest (OOH-CA) nearly doubles when laypersons trained in cardiopulmonary resuscitation (CPR) are also trained in and provided access to automated external defibrillators (AEDs).
The survival benefits of AEDs in the hands of public safety workers, such as flight attendants, security guards, and casino employees, has been well documented. However, to date, no randomized trial has been conducted to test whether nonmedical, true laypersons who do not have a formal duty to treat patients in medical emergencies can save more lives when they are trained and equipped to use AEDs, in addition to just calling 911 and performing CPR. The PAD trial, funded by the National Heart, Lung, and Blood Institute, in partnership with the American Heart Association, is the largest prospective, randomized, controlled clinical trial undertaken to examine this specific issue.
PAD was a massive undertaking in which almost 20,000 volunteers were trained, said Chairman of the PAD Steering Committee Joseph P. Ornato, MD, Department of Emergency Medicine, Virginia Commonwealth University/Medical College of Virginia (Richmond).
Dr. Ornato presented the results at a late-breaking clinical trials session at the American Heart Association Scientific Sessions 2003.
Standard CPR vs CPR plus AED
More than 1600 AEDs were placed at 993 sites in 24 regional sites in North America. Individual community units considered at high risk for OOH-CA were randomized to train layperson volunteers in either a 2-hour course that taught CPR only (recognition of cardiac arrest symptoms, instruction to call 911, and performance of CPR) or in a 4-hour course that trained volunteers in CPR, as well as in how to use an AED within a 3-minute time window. Additional retrainings were conducted at various planned intervals. Volunteers for the study had to have no duty to treat in medical emergencies (ie, physicians, nurses, emergency medical technicians, firefighters, and police were excluded).
Dr. Ornato reported that 24% of units were in shopping malls; 24% were placed in recreation centers; 15%, in residential units; 14%, in hotels, factories, and transit centers; 9%, in theaters and other entertainment centers; and the remainder in community centers and office buildings.
All PAD sites were within a “15 minute range of EMS [emergency medical services] response; we did not include rural or remote sites.” Follow-up averaged just over 21 months.
Distinguishing “presumed” from “definite” cardiac arrest
Dr. Ornato noted that the study design opened the door for ascertainment bias, in that an episode of sudden cardiac arrest could be misinterpreted. Dr. Ornato used the example of an elderly man found unconscious in a pool. If responders use an AED that documents ventricular fibrillation and efforts fail, his death is classified as a cardiac arrest. However, in the same scenario, if responders only use CPR and their efforts fail, the death is classified as a drowning.
To overcome the potential for this bias, an adjudication committee blinded to the intervention was used to distinguish presumed vs definite cardiac arrest. Cardiac arrest was classified as definite if ventricular fibrillation/ventricular tachycardia or asystole was identified by the AED or by EMS or if the victim was found unresponsive with no pulse and died after CPR.
PAD results show AED use doubled number of survivors
Over the study period, investigators reported that there were significantly fewer incidences of definite OOH-CA in the CPR-only group vs the CPR + AED group (103 vs 129, respectively; P = .041). This significant difference was expected, Dr. Ornato told attendees. The majority of OOH-CA events (85%) occurred at public places (the majority in recreation, shopping, and entertainment facilities), and 15% of OOH-CAs occurred in private residencies (eg, apartment buildings or gated communities). Dr. Ornato noted that clinical and demographic characteristics were well-matched between the 2 groups; victims were predominately white, male, and aged 70 years.
Investigators found that the number of survivors of OOH-CA through hospital discharge, the study’s primary endpoint, was nearly doubled in the CPR + AED group, compared with CPR only units (Table). As noted by Dr. Ornato, the rate of overall survival was still disappointingly low in all patients.
Table. PAD: Primary Endpoint
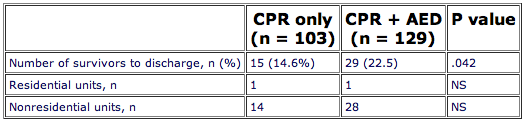
AED indicates automated external defibrillator; CPR, cardiopulmonary resuscitation
Disappointing survival rates for home defibrillation
Dr. Ornato said that 15% of the AEDs were placed in residential units, usually “large apartment complexes or gated communities in which the residents were 50 or older.” However, these home units only accounted for < 5% of survivors, and outcome was not influenced by the presence or absence of an AED; both the CPR-only and CPR + AED groups had only 1 survivor to hospital discharge when cardiac arrest occurred in a residential unit.
Dr. Ornato cautioned against extrapolating the PAD findings to the home defibrillation setting. In the residential units, AEDs were not confined to individual apartments. Instead, they were centrally located in a public setting, in which a trained volunteer would have to retrieve the device and return to the apartment where the victim lived in order to deliver therapy. According to Dr. Ornato, the large ongoing Home AED Trial (HAT) will specifically address the role of in-home defibrillation to determine its role in preventing sudden cardiac death.
PAD fails to answer all questions, but take-home message still important
Roger D. White, MD, Mayo Clinic (Rochester, Minnesota), hailed the PAD trial as “truly a landmark trial” that has been eagerly anticipated. But he said that the number of arrests was lower than had been anticipated and that “the data don’t tell us how many patients had a rhythm not treatable by AED.” Additionally, he said that the study failed to identify AED locations where the devices were most useful.
Richard L. Page, MD, Robert A. Bruce Professor and Head, Division of Cardiology, Department of Medicine, University of Washington School of Medicine (Seattle), told Medscape CRM that he did not originally support the PAD study because he thought it was unnecessary. He said his work in Seattle subsequently convinced him that AEDs could significantly reduce out-of-hospital sudden cardiac death.
“AEDs have been shown to be effective in non-randomized series such as in casinos and our study with airlines,” Dr. Page said. “This report [PAD] represents the largest randomized trial of AED use by trained volunteers, and the study confirms that the AED improves the chance of survival from sudden cardiac arrest.”
Nevertheless, the take-home message is still quite clear. Speaking at an AHA press conference where the PAD results were discussed, Raymond J. Gibbons, MD, Chairman of the American Heart Association Committee on Scientific Sessions Program and Arthur and Gladys D. Gray Professor of Medicine at Mayo Medical School (Rochester, Minnesota), said that the study clearly demonstrated “the value of training people to use AEDs in the kinds of public places that were described.” Dr. Page agreed, adding, “It is time to fully deploy AED programs in places where numbers of people gather.”
By Peggy Peck
Reviewer: Albert A. Del Negro, MD
Copyright © 2003 Medscape.